|
Keep an open mind on traditional medicine, docs told
Kuala Lumpur:
Doctors have been urged to keep an open mind on the use of traditional and complementary medicine in keeping with
global trends. Health
Minister Datuk Chua Jui Meng said the philosophy and the policy of the world Health Organization was to see greater intergration between
traditional and complementary medicine.
" It is the policy of this ministry to promote traditional and complementary medicine which may or not be included
in the health supplements.If we were to exclude that , it would not be healthy and not in line with development in the rest
of the world - especially the developed countries, so we hope everyone will keep an open mind, " he told a press conference
yesterday. Chua added that the ministry's director-general would meet doctors to discuss the issue. On Monday Malaysian Medical
Association president Dr. N. Arumugam was quoted as saying that the association had banned doctors from selling health supplements.
since last April. The Malaysian Dietary Supplements Association ( Madsa ), however, expressed surprise over the ban as it
implied that supplements were detrimental to health. Madsa said supplements that had been on a typical doctor's prescription
list included iron for anaemic patients, calcium for osteoporosis and folic acid for pregnant mothers. Prestigious medical
journals such as the Journal of the American Medical Association and New England Journal of Medicine had also supported the
use of health supplements, it added.
The Star, page 8, Saturday 7, February 2004
E-mail : editor@thestar.com.my
" We hope everyone will keep an open mind.
" - The former Health minister,
Datuk Chua Jui Meng of Malaysia
After 25 years
of struggles, homeopathy has been recognized by Ministry of Health Malaysia in year 2000. Thanks to the former Health Minister, Datuk Chua Jui Meng of Malaysia
The formation of the Homeopathy Faculty
.
http://www.geocities.com/fakulti/hm.htm
" Classical homeopath
does not include any other surrounding or possible alternative medicines like vitamins, minerals, herbs or whatever. ... And
sometimes, a homeopathic remedy cannot cure a problem--for example, if your diet does not include a lot of salads or greens,
you might have an vitamin A deficiency and complain of poor night vision....the only thing that will help that is to change
your diet to include these foods, and/or take a vitamin A supplement. Homeopathy SOMETIMES can help you change your eating habits. But because the soils and veggies/fruits are depleted and no longer have
the levels of vitamin they used to before 1960, we are getting depleted and need supplements, " Eileen Nauman, my Cherokee
American friend, well known internationally as a writer and Homeopath in complementary
and alternative medicine, commented, in our Athena forum a few years ago.
I
recall those difficult years when I had to improvise very simple ways to manage emergency cases while practising in remote
areas in the state of Johore, Malaysia, when the nearest hospital was miles away. Droplet feeding a succussed
preparation from the patient's vomitus in accidental poisoning was a desperate homeopathic procedure in jungle medicine but
not in orthodox medicine.. There was no time for detailed history -taking. Slipping some crashed homeopathic granules of Antimony
Tartarate 6x into a gasping cyanotic child's mouth, with respiratory problems before the frantic rush to the nearest hospital,
was another emergency measure. My limited supplies of homeopathic medicine , which included principally the
homeopathic specifics for soft tissue injuries and bony trauma :Hypericum, Arnica, Natrum Sulph,
Calendula , Ruta, Symphytum, Ferrous Phos, Silica, Bellis Perennis
and the like , were obtained from Sungai Patani, friendly homeopaths in Kuala Lumpur and Kota Baru,in Kelantan.
I still recall the kindly homeopath from Kota Baru, Dr.Nik, now professor, who sent me Ringgit 200 worth of homeopathic
medicine on credit which I managed to pay off with the small collections from poor patients. Life has taught me
the best under such straitened circumstances. I seldom used steriods. I sparingly prescribed antibiotics because I resorted
to the homeopathized specifics for cleansing and the management of badly infected cuts and wounds with
wild honey dressing of the injuries.I found that diabetic ulcers healed fast with raw honey dressing. It was not safe
to keep tetanus toxoid because the supply of electricity in the village was erratic. Instead, I prepared Hypericum and Ledum
globules, which were adminstered orally under the tongue, for the prophylaxis of Tetanus. "
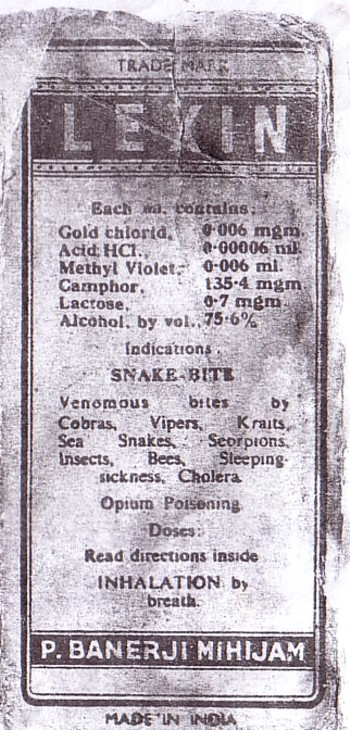
Lexin " , a snake -bite preparation developed by Dr. Parimal Banerji 's father,Maharshi
Pareshnath Banerji, had saved many lives. It was administered by olfaction.I saved enough money, with
skipped meals to buy Homeopathic Books from the Jain Homeopathic Publishers in India.The determined
will to learn a new discipline of medicine, Homeopathy, which is not taught in Orthodox Medicine spurred me
on to trudge wearily, inspite of all the deprivations that I have been subjected to, the lonely Way in search of the
Holistic truth , a lonely and non-lucrative path . I still treasure those books which I have faithfully
preserved till this very day. Though these homeopathic
books
are torn and tattered now, they are still,my constant sleeping companions. A far cry from those hectic days of
jungle medicine ,however, whenever, I pick up one of them for reference with my hands,it is like shaking the hands of old
friends and teachers. Though not an institutionally qualified homeopath, I studied and researched the Holistic
Principles of Homeopathy Nature 's way with a sound grounding of the Basic Medical Sciences taught me in Medical College. My naive patients are/were my best teachers and I gleaned from them the true meaning of the WHO 's holistic
trio of healing: Physical, Emotional and Spiritual. They were graphic projections of living drug-pictures
of symptoms in totality. They taught me Homeopathy.
Enabling
the patient to breathing 'in' and 'out' of a make-shift perforated paper bag of " bad gas " rather than an
oxygen mask for oxygen, for better carbon dioxide and exhaled Nitric Oxide retention , was a life-saving
measure to maintain vasodilation to provide oxygen for life maintenance to the anoxic child during the journey to the nearest medical institution .
(
Nitric oxide is a potent endothelium-derived vasorelaxant substance and an inhibitor of smooth-muscle-cell
growth . Nitric oxide is produced in various cell types by the action of an enzyme, nitric oxide
synthase and L-arginine.
Inhaled NO appears to be an ideal treatment for hypoxemia in patients with acute respiratory distress syndrome
because it selectively increases perfusion to portions of the lung receiving ventilation. However, because most patients with
acute respiratory distress syndrome do not die from hypoxemic respiratory failure, but from multisystem organ failure, inhaled
NO may not improve final outcome. Randomized clinical trials have reported temporary improvements in arterial oxygenation
but no significant differences in outcome between patients who received inhaled NO and those who received placebo gas.Despite
these observations, inhaled NO may allow clinicians to use less-injurious ventilatory strategies (e.g., by reducing the inspired
oxygen concentration), and this may reduce toxic effects and morbidity. In addition, inhaled NO may prove invaluable for the
minority of patients in whom severe oxygenation defects are the primary cause of death. The only area where NO has proven
efficacy is in infants with persistent pulmonary hypertension, where it has been found to improve systemic oxygenation and
decrease the need for extracorporeal membrane oxygenation.
The benefit (or harm) of NO will most likely be secondary to its immunological effects. Inhaled NO is capable of modulating
neutrophil chemotaxis, adherence and activation,both locally and in nonpulmonary vascular beds after reperfusion injury; therefore,
future studies will likely evaluate its immunomodulating potential in patients who are at risk for acute lung injury and reperfusion
injury syndromes.
As suggested in the Buteyko Protocol, it seems that breathing air with a 8% CO2 content, not only raises the
body ' s pH and oxygen level but also eliminates pulmonary infection, has favorable outcome for patients of cardio-vascular
accidents, for the asphyxiated and the brain-damaged. )
INHALED NITRIC OXIDE GAS THERAPY and ARDS ( Acute respiratory Distress Syndrome )
Posited as
a Emergency measure in Sars and Avian Influenza
This
writing is intended to briefly introduce
ARDS patients, their families, and significant
others, with the properties of nitric oxide
and the clinical implications associated with
the use of this gas. Nitric oxide should(NO) not be confused with nitrous oxide (N20), the mild anesthetic
often used by dental
professionals that is more commonly known as "laughing gas." As a matter of fact, nitric
oxide was known as a common environmental
I pollutant and contaminant during the
manufacturing process of nitrous oxide. NO is
normally manufactured from the
reaction of
sulfur dioxide with nitric acids. Nitric
oxide
is a component of smog that can be measured in
urban area air at 10 to 100 parts per billion
(ppb), is naturally produced in the body in the upper and lower airway at 100 to 1000 ppb,
and is present in cigarette smoke at 400 to
1000 parts per million (ppm). Clinical
research found that the concentration
of
exhaled NO is increased during exercise and in patient's with
asthma.
Inhaled NO is a relatively new United States
Food and Drug Administration (FDA)
investigational drug and numerous
facilities
are involved in clinical trials utilizing this
gas. Until approved by the FDA, its use is
limited to
those facilities that have gone
through the application process for drug
evaluation and research and have been granted permission (known as an Investigational New
Drug [IND] number) to conduct such studies utilizing NO. In addition, an informed consent
procedure must be obtained from each patient or legal representative prior to the administration of NO.
Physiology of ARDS
A
limited review of the pulmonary disease , ARD , is necessary to gain an understanding of the way in which NO affects
this pulmonary
ailment.
Patients with ARDS, whether precipitated by
inhalation of vomited stomach contents
(aspiration), injury, pneumonia, inhalation of
toxic substances, or a severe infection
somewhere in the body (sepsis), usually all
have high blood pressure in the vessels
leading to and around the lungs (pulmonary
hypertension.) Also, under normal conditions,
if the tiny air sacs in the lung (alveoli) do
not receive enough air or are collapsed
(atelectasis), the blood vessels supplying
these alveoli will constrict (become smaller
or narrower). In ARDS however, these collapsed
or underventilated alveoli continue to receive
full blood supply from the surrounding blood
vessels (capillaries). Since these collapsed
or underventilated alveoli are not receiving
oxygen, they are not capable of providing
oxygen to the blood stream. The net effect may
be a severe reduction in oxygen levels in the
blood stream.
Basic Science
Certain substances that occur naturally in the
body exert control over blood flow in and
around the lungs. These substances can cause
blood vessels near the lungs to dilate (become
wider or larger, vasodilation). They produce
this vasodilation by causing cells lining the
blood vessels to produce the gaseous product
NO. NO accounts for the physiological effects
of vasodilating drugs such as nitroglycerin; a
drug commonly used to treat high blood
pressure. Recent studies have found that
excess NO production in the body plays a role
in the massive vasodilation and low blood
pressure associated with septic shock
syndrome.
Since NO exists in a gaseous form, it can be
applied to the pulmonary vessels by
administering it as an inhaled gas. What this
means, is that when NO is inhaled, it
selectively dilates blood vessels in only
those lung segments that are actively
participating in gas exchange (oxygen & carbon
dioxide) at the alveolar-capillary level. In
other words, this increases the blood flow to
areas of the lung where oxygen is being
provided and thus improves oxygen levels in
the body. This is known as
ventilation-perfusion (V/Q) matching.
However, the lower respiratory tract contributes
substantially to exhaled NO. Direct sampling
via
fibreoptic bronchoscopy in asthmatic patients
shows a
similar elevation of NO in trachea and main bronchi
to that recorded at the mouth, thus indicating that
the elevated levels in asthma are derived from the
lower airways.
Biological relevance of exhaled nitric oxide.
Concentrations of NO present in expired air are
considered to be too low
to be of physiological
relevance [16, 17]. That is to say that nM concentrations
of NO are unlikely to have substantial bioactivities
in the lung
(as NO) where there is continuous
exposure to a high flow
rate of mM haemoglobin
concentrations which avidly bind NO . However,
NOS activation does not result in the formation
of NO alone . It may form a variety of nitrogen
oxides with a broad range of bioactivities ,
such as nitrate, nitrite (NO2 and peroxynitrite.
NO was not the first drug discovered that
causes pulmonary vasodilation. There are
several other drugs that are known
vasodilators that have been on the market for
years. These include the aforementioned
nitroglycerin and nitroprusside. The
shortcoming of these types of drugs is that
they increase the pulmonary blood flow to all
lung segments, including those that are not
well ventilated. This further inhibits oxygen
delivery to the blood stream because
capillaries are dilated that are in contact
with alveoli that are not providing or do not
contain oxygen.
Inhaled nitric oxide (NO) dilates only
ventilated alveoli, an outcome that improves
V/Q matching. (From Lunn R: Subspecialty
clinics: Anesthesiology; Inhaled nitric oxide
therapy. (Mayo Clin Proc 1995; 70:247-255;
with permission.)
After the NO is inhaled and passes through the
lungs and into the patient's blood stream, its
effects are quickly deactivated. This is
because NO quickly reacts with the
iron-containing pigment of the red blood cell
that functions to carry oxygen from the lungs
to the tissues (hemoglobin). Hemoglobin
inactivates NO and thus when it is carried to
the rest of the body, it does not cause
vasodilation to blood vessels beyond the lung
area. This is in stark contrast with some of
the other pulmonary vasodilator drugs that not
only cause vasodilation of blood vessels in
and around the lungs, but also cause
vasodilation throughout the body. This can
potentially lead to a serious decrease in a
patient's blood pressure.
Gas Delivery Systems
As mentioned earlier, the way in which this
drug is administered is simply by providing
the gas for the patient to inhale. There are a
variety of delivery systems that are presently
in use. These either encompass a homemade or
"rigged" system or a commercially available
delivery system. They can provide gas delivery
via a ventilator circuit, a facemask, or a
nasal cannula.
The basic design and goal of each system is to
provide a system for safe gas delivery and
precision gas analysis or monitoring. If
delivering the gas through a ventilator,
either a continuos or intermittent flow of NO
is fed into the inspiratory limb of the
ventilator tubing. The rate of NO gas flow is
controlled to maintain the desired levels of
NO. Prior to the patient connection of the
ventilator tubing, a sensor or sample line is
connected to an analyzer that displays NO, NO2
(discussed in further detail later) and
possibly oxygen levels. Usually the displayed
NO and NO2 readings are measured in parts per
million.
Safety Concerns
As with any drug, there are legitimate safety
and toxicity concerns regarding the use of
inhaled NO. Inhaling very high levels of NO
(5,000 to 20,000 ppm) can be lethal causing a
severe and acute accumulation of fluid in the
lungs (pulmonary edema) and methomoglobinemia
(described below). However, there is little
evidence of such toxicity when the
concentration is kept in the normal
concentration range (1 to 80 ppm). Animals
have breathed the gas in concentrations of 10
to 40 ppm, for six days to six months, without
evidence of toxicity.
Virtually all patients receiving NO will also
be receiving oxygen (O2). ARDS patients
usually require high levels of O2. The
by-product of NO and O2 yields nitrogen
dioxide (NO2). NO2 is a highly toxic chemical.
Although OSHA has set the safety limit for NO2
at 5 ppm, some investigators have found that
prolonged exposure to even 2 ppm of NO2 can be
injurious to the lungs. The amount of NO2
produced is dependent upon the levels of NO
and O2 and the amount of time they are
combined together prior to inhalation.
Therefore, the lowest dose of NO and lowest
concentration of O2 that achieve the desired
effect are used. NO is usually fed into the
ventilator tubing as close to the patient as
possible, limiting the mixing time between O2
and NO.
All delivery systems monitor NO2 levels
continuously. Newer delivery systems have been
designed to limit NO2 production or inhibit
its delivery to the patient, but situations
may occur where the NO dose, the O2
concentration, or both, may have to be
reduced.
One of the potential adverse side effects for
patients receiving inhaled NO is the formation
of methemoglobin. Methemoglobin is hemoglobin
that cannot release the oxygen its carrying,
nor can it combine with more oxygen.
Therefore, it impairs the blood's ability to
deliver oxygen to the tissues. This is a rare
complication because the body contains certain
chemicals and enzymes that convert
methemoglobin back to hemoglobin.
Nevertheless, blood levels should be closely
monitored.
Patient Outcomes
Virtually since the discovery of NO for
medical use in the mid-to-late '80s, it has
been trialed on patients with acute
respiratory distress syndrome (ARDS). Numerous
formal studies have been completed that
examined the effect NO had on ARDS patients.
Virtually every study found that inhaled NO:
1) induced a redistribution of blood flow in
the lungs to areas that were well ventilated,
2) reduced the blood pressure in the arteries
surrounding the lungs, and 3) improved oxygen
levels in the blood. How NO is capable of
producing this effect was described earlier.
This research has also found that not every
patient responds to inhaled NO in the same
manner. Some patients have an almost immediate
positive and recognizable response. While
others have a limited response. Some studies
have found that only about one-third of
patients with ARDS due to sepsis had a
positive response to inhaled NO. Among other
factors, patients who had high blood pressure
in the arteries near the lungs and who
demonstrated a positive response to PEEP
(positive end-expiratory pressure from the
ventilator), appeared to be most likely to
have a positive response to inhaled NO. For
some patients, the positive response to
inhaled NO appears to last for only hours to
days while others respond positively for
weeks. The reason for this phenomenon is still
being investigated.
As mentioned earlier, ARDS patients are
usually receiving high concentrations of
oxygen. High-level oxygen administration for
an extended period of time (usually > 72
hours) is well known for its pulmonary
toxicity. Since NO has been proven to improve
oxygen levels in the body, numerous clinical
studies have found that adding NO to a
patient's inhaled gas allowed a reduction in
the oxygen concentration being delivered to
the patient, and thus a concomitant reduction
in possible toxicity to the lungs.
So how has NO affected mortality and length of
intensive care unit or hospital stays? Since
NO is a relatively new medical adjunct, there
have been only a limited number of studies
that have tracked and reported patient
outcomes. Most research has focused on the
physiological effects and patient response to
inhaled NO.
In the largest study to date, 177 patients
diagnosed with ARDS, from various test sites
throughout the country, were randomized to
receive NO or a control gas (placebo). Results
of this study were: 1) an initial increase in
oxygenation allowed a reduction in O2
concentration, 2) there were no differences
among the groups receiving NO and the placebo
with respect to mortality rate, the number of
days alive and off mechanical ventilation, or
the number of days alive after meeting a
criteria for removal of mechanical
ventilation, 3) however, the percentage of
patient's alive and off mechanical ventilation
by day 28 that were receiving 5 ppm of inhaled
NO, was higher (62% vs. 44%) than the placebo
group. Even though most other studies were
conducted using much smaller patient
populations, almost all had the similar
findings of improved gas exchange, but no
effect on mortality.
The difficulty in analyzing the success or
failure of patient outcomes (mortality and
length of stay) for patients with ARDS is that
the reversal of lung failure may be obscured
by the development of other organ system
malfunctions that often may occur with ARDS.
Studies continue to address the use of NO to
improve the overall prognosis for ARDS
patients. Actual studies that are underway
include methods of predicting which patients
will respond positively to inhaled NO, the
optimal dose concentrations, patient
positioning during NO delivery, and
examination of potential long term toxicity.
Research has been proposed that would make
comparisons of NO delivery devices on patient
outcomes, and standardization of ventilator
management during NO administration.
By Dean Miller, BSRC, RRT
Education Coordinator
Respiratory Care Services
St. Luke's Medical Center
Milwaukee, WI
Under such straitened circumstances, I witnessed the foreign-body extruding effect of potentised Silica in healed injuries
still harbouring the retained debris. The extruded objects [ tiny glass pieces and wooden splinters] were palpable over the
skin. My patients from the jungle fringes in Kahang, Johore shared with me their folklore steeped in traditional medicine.It could be that the memories of the sounds and voices [ Nature's silence ] of the
rainforests where I spent most of my childhood, that had lured me to trudge the lonely Way searching for holistic
truths.
What mainstream medicine considered as healed
on the radiological evidence of calcification of the TB tubercles in the lung fields, seen as opacities is but an evasive
and protective mechanism evolved by the Tubercular Bacilli to escape chemical destruction and immune surveillence. This protective
phenomenon is observed in the Nano-Bacteria which produce a similar cellular calcium coating or a biofilm which prevents
the microbes from destruction by the immune cells or antibiotics. Nano-bacteria are immune to anti-microbials. The criterion
of recovery from TB is bacteriological and not radiological. I rely more on the bacteriological staining from sampling of
the saliva or a gastric aspiration. It has been observed that Cell Salts can cause morphological alterations in microbial
colonies. Potentised quartz [ silica ] causes a flaring up of old calcified TB lesions in the lungs, in the process of extrusion.
This phenomenon has been observed by astute holistic researchers. In Biological Transmutation, Prof Kervran [ University of Paris ] showed that the assimilated calcium is not utilised by the body as
such but is converted to magnesium which is stored in the body.This calcium-transmutated Magnesium is reverted back to calcium
to meet the body's demands as needed. In his classical experiment, Prof Kervran demonstrated
the Biological Transmutation of Quartz [silica] to Calcium present in the egg-shell with different chicken-feeds.The transmutated
calcium is the biological calcium which has its specific vibratory signature. The dynamised silica unmasks the non-biological
calcium coating of microbes by causing vibratory disresonance extracellularly and intracellularly,thus exposing the pathological
microbes to the immune system of the body.. A flaring-up of the so-called healed calcified TB lesion is instituted by immune
cells as a homeostatic response to rid the body of foreign matter. This is part of the rationale of flaring-up and extrusion
of calcified TB lesions and other foreign bodies in the human body observed by earlier homeopaths and holistic researchers.. As a matter of fact, potentised silica has antibiotic properties. I have resorted
to homeopathized Silica which is one of the essential tissue salts of Schuessler, for management of chronically discharging
infected lesions with a dosage of 2 drops of Silica 200x on the tongue with a monthly review. These lesions heal with proper
dietary advice and nutrient supplements. I have compiled some of the scraped notes on rural practice in holistic medicine years ago on Nutritional Science. I have uploaded the pages to a website.. The pages
have an old fashion typeface but I hope the messages in these faded pages are legible in the webpages.
Very few would trudge the lonely path the way I did. I had suffered and
ran the gamut which many of my pioneering teachers of holistic medicine and allied sciences had experienced. The reawakening
was rejuvenating and the realization
of my cherished dream that eventually the medical establishment in Malaysia would resonate with Mother Nature is well worth all the illusory deprivations that had beset me and the shattering experience
of holistic reawakening.
What is Vibrational Medicine ?
Stefanatos ( 1997,228 ) tells us that the " electromagnetic fields (EMF)emanating from bacteria,viruses and
toxic substances affect cells of the body and weaken its constitution." So the vital force is identified quite explicitly
with electromagnetic fields and said to be the cause of disease. But somehow the life energies of the body are balanced by
bioenergetic therapies. " No antibiotic or drug, no matter how powerful, will save an animal or human if the vital force of
healing is suppressed or lacking ." ( Stefanatos 1997, 229 ) So health or sickness is determined by who wins the battle between
good and bad electromagnetic waves in the body.
Electronic and Magnetic medicine is going to be the future medicine. The average frequency of the human body
during the day is between 62 and 68 cycles each second.If it drops below this rate,the immune defence system will start to
shut down.
Cold symptoms appear at 58 cycles,
Flu at 57, Candida at 55, Glandular Fever at 52,
Cancer at 42 cycles each second.
Dr. Young and Bruce Tainio [ Cheny University. WA. USA]
Anthroposophic Medicine
A unique specialty is Anthroposophic Medicine. With
the founding of Homeopathy by Samuel Hahnemann in the early 19th century, and of Anthroposophic Medicine by Rudolf Steiner
in the early 20th century, Medicine has rediscovered some of its spiritual and holistic roots.
On one hand, Anthroposophic Medicine is thoroughly modern requiring its practitioners to be fully qualified
MDs or DOs (Osteopaths) with a solid grounding in mainstream medicine. On the other hand, Anthroposophic Medicine seeks to
change our modern view of the human being as a marvelous machine to a renewed holistic understanding of ourselves as fourfold
beings: spirit, soul, life forces and our physical body.
The Anthroposophic physician or therapist strives to develop his or her intuitive grasp of the spiritual dynamic
at work in every illness. The practitioner's training to access insight that can serve the patient's healing is not only a
scientific endeavor, but an artistic and moral endeavor as well.
Today, Medicine is at a crossroads. Although it has successfully contributed to the diagnosis and treatment
of disease for the last four decades, it has not been as successful in promoting healthy aging. The movement from disease-centered
care to patient-centered care is provoking new questions relative to health and vitality across the lifespan.
Sources: Philip Incao MD ; Larry Eckstein,
MD, and Lisa Bassow, MD.

The following faded typeface pages are the recordings of a Memory
Replay of the Sounds and Voices of Nature's Silence in a Malaysian Rainforest, where I spent most of my earlier childhood
in the company of
freely roaming wild creatures with luxuriant plants and trees. In memory of
the deafening pattering of rain on zinc roof, the howling wind through
unclosed windows, the dripping sound of rain-drops, the ear-splitting thunder and lightning in
a tropical storm, the muscial sound of nocturnal insects and
the ocassional distant roar of a foraging tiger ( Nature's Silence ) , under a swinging electric bulb
caused by eddying wind currents, I framed my thoughts in these notes. One is closest to
Mother Nature and Nuture when one is attuned to Nature's Silence.
Nutritional Science (1991)
- Dr. FHLew
Kahang
, Johor
Malaysia
Village Medicine
All these years of practice have taught me that med-
icine is holistic. Doctors do not cure patients; we merely
help them towards homeostatic equilibrium. Nature does
the rest. Treating the symptoms without rooting out the
cause is not holistic medicine. In fact, this is what we
have been doing all the time in orthodox medical practice.
In reality, no drug has ever healed a person. Hippocrates
stated :
"
The body heals itself; the physician is only
Nature's assistant. "
- Lew
Synthetic anti-microbials usually drive the " taint" or symptoms deeper in the body parts and may disappear for sometime
but there is always recurrence.The symptoms are merely suppressed without removing the cause of the of the disease.
" The 'disappearance' of a particular
germ from the culture does not mean that the germ is dead; it only became invisible due to its transformation into an invisible
form. That means the host organism is now in a cancerous state.... Today's mainstream medicine is governed by consent of opinions
rather than hard scientific evidence. This is the reason why false and fraudulent teachings can survive even though the truth
has been known for a long time."
- Dr. Karl Horst Poehlman,Australia
Pasteur ,on his death-bed, is said to have made the
heretical statement:
" The bacteria are nothing, the terrain is everything.
"
| |
|
|
To those men in every science and art who are investigating the properties of the chemical elements,their structure
and
their application for the betterment of the physical temple of man's well-being. To know the dust of the earth in the form
of vitamins,enzymes,protein,starches,fats,
prostaglandins and mineral supplements in foods is to understand the source
in nature from which health and well-being spring.
- Bernard Jansen
What is Biodynamics?
| Dr. Benard Jansen |
|
| A pioneering researcher in Holistic Nutrition |

( please continue from Introduction
and Page 1 )....
.... -lest eating customs. Thus, we are what we eat,drink,breathe
or associate with. An understanding of herbs and herbal
products projects us into a dimension where knowledge is
inter-related, demonstrating the universality of creation
in Nature's alchemical laboratory and the operation of the
Universal Mind. The study of herbal wholistics and isolates
gives us a better appreciation of the ethnobotanical, socio-
economic and mystico-cultural influences in anthropology,
which have contributed considerably to the evolution of
folklore, traditional medicine, medical sciences and in part-
icular, organic chemistry. The philosopher, Hegel, stated:
" All knowledge is one. If we can know everything
about
one thing, we will know all. "
Village Medicine
All
these years of practice have taught me that med-
icine is holistic. Doctors do not cure patients; we merely
help them towards homeostatic equilibrium. Nature does
the rest. Treating the symptoms without rooting out the
cause is not holistic medicine. In fact, this is what we
have been doing all the time in orthodox medical practice.
In reality, no drug has ever healed a person. Hippocrates
stated :
" The body heals itself; the physician is only
Nature's assistant. "
The awakening to this time-honoured philosophy is
stimulated by my having to work in unfavourable conditions
in the outskirts of the Kahang rainforests, Johor, Southern Malaysia.
This town village is subjected to periodic floods, causing
overflowing from blocked drains and sewage, fouling the well-
water which is not chemically treated. The well water is
very acidic with a pH about 6 [ potable range is pH 6 - 10.5 ]
The low pH of the drinking water is sure to affect the blood pH.
How this biochemical aberration is going to affect the paediatric,
geriactric and the pregnant population in Kahang? How the low
blood pH is going to affect those with chronic medical problems
and its inter-
Page 2
actions with mediciation ? The health Office is not of much
help. Dermatological problems are rampant amongst those
exposed to pesticides, herbicides, chemical fertilizers,
poisonous plants and trees. My library which includes a number
of books on herbal medicine and herbal write-ups gave me
the first clue and solution. Alfalfa [ Medicago sativa ], a
chlorophyll-containing food nutrient which is capable of alkalizing
and detoxifying the blood. Out of a sincere and urgent
need to relieve and to avert further toxic build-up in my
patients, I fell on my academic knees to enlist Nature's
assistance. This is my first encounter with traditional medicine,
a blend of East and West, using simple adaptogens daily for
management of medical problems.
According to Lazerev,Brekhman
and Bardymov of the USSR Academy of Sciences , an adaptogen is anything
that " increases the non-specific resistance of an organism"
to stress or other deleterious environmental factors [ injury,
infection, disease or anxiety ]. Adaptogens normalise bodily
processess," increase efficiency both after a single ( stimulant action)
or prolonged ( tonic action ) administration and are non-toxic.
The term adaptogen is used by herbalists to refer to a natural herb product that is
proposed to increase the body's resistance to stress, trauma, anxiety and fatigue. In the past, they have been called rejuvenating
herbs, qi tonics, rasayanas, or restoratives. All adaptogens
contain antioxidants, but antioxidants are not necessarily adaptogens
and that is not proposed to be their primary mode of action.[1]
The concept
of adaptogens dates back thousands of years to ancient India and China, but modern study did not begin until the
late 1940s. In 1947, Nikolai Lazarev defined an adaptogen as an agent that allows
the body to counter adverse physical, chemical, or biological stressors by raising nonspecific resistance toward such stress,
thus allowing the organism to "adapt" to the stressful circumstances.[1]
In 1968, Israel I. Brekhman , PhD, and I. V. Dardymov formally gave adaptogens
a functional definition, as follows:
1.
An adaptogen is nontoxic
to the recipient.
2.
An adaptogen produces
a nonspecific response in the body—an increase in the power of resistance against multiple stressors including physical,
chemical, or biological agents.
3.
An adaptogen has a normalizing
influence on physiology, irrespective of the direction of change from physiological norms caused by the stressor.
Under this definition,
adaptogens would be nontoxic in normal doses, produce a general defensive response against stress, and have a normalizing
influence on the body.[1]
It is claimed that adaptogenic herbs are unique from other substances in their ability to balance endocrine hormones and the immune system, and they help the body to maintain optimal
homeostasis.[1] Adaptogens are proposed to have a normalizing
effect on the body and to be capable of either toning down the activity of hyperfunctioning systems or strengthening the activity
of hypofunctioning systems. However, they are also proposed to be functional at the level of allostasis, which is a more dynamic reaction to long
term stress, lacking the fixed reference points of homeostasis.[2] - From
Wikipedia, the free encyclopedia
Adaptogens Therapeutic uses
Alfalfa
Blood alkalizer
[ Medicago sativa ]
Blood detoxifier
Gastritis
Nutrient
Aloe Vera
Superficial wounds
Burns
Acne
Ginger Root
Motion Sickness
[ Zingiber officinale ]
Car Sickness
Morning Sickness
Dizziness
Page 3
Adaptogens
Therapeutic uses
Hypercholesterolaemia
Yeast Infection
Shitake & Reishi Mushroom Anti-oxidant
( contains organic Germanium )
Smoking
Propolis
URT Infection
( a bee-hive extract )
Immunostimulant
Antibiotic
Germ Rice
Nutrient
Constipation
Royal Jelly
Underweight infants
Morning
sickness
Arthritis
Hypertension
Menopausal syndrome
Neurasthenia
Insomnia
Diabetes
Bee Pollen Nutrient
Honey
Nutrient
White sugar substitute
Blood alkalizer
Anti-septic
Vitamin C with bioflavinoids
Anti-oxidant
( Rutin and Hesperidin )
URT INfection
1000 mg acid free
Esterified vitamin
C
Arthritis
( Neutral
550 mg )
URT Infection
Anti-oxidant
Butcher's Broom
Haemorroids
( Ruscus aculeatus)
Page 4
Adaptogens Therapeutic
uses
Varicose veins
Lecithin with Vitamin E
Hypertension
Hypercholesterolaemia
Haemorroids
Bedsores
Psoriasis
Scaling and fissuring
Nappy rash
Eczemza
Echinacea augustifolia
Antibiotic
Gingko biloba
Stroke
Deafness
Tinnitus/Vertigo
Intermittent claudication
Comfrey ( Symphytum offinale )
Respiratory Tract
with Fennygreek ( Trigonella
Infection
foenum-graecum )
Unpolished Rice Enzyme
Migraine
Asthma
Anaemia
Obesity
Neurasthenia
Nutrient
Dong Quai
( Angelica sinesis )
Menopausal
syndrome
Menstrual irregularity
Anaemia
Ginseng
Hangovers
( Panax ginseng )
Nervous disorders
Anaemia
Hypertension
Hypotension
Diabetes
Page 5
Adaptogens
Therapeutics
Hepatitis B Vaccine with
Hepatitis B
pre-S antigen
Lactobacilli
Gastroenteritis
1. Acidophilus
Constipation
2. Bulgaricus
Halitosis
Autointoxication
Flatulence
Bran High Fibre
Constipation
1. Wheat bran
Obesity
2. Apple
pectin
Hypercholesterolaemia
Colitis
Passion flower
Insomnia
( passiflora incarnata )
Nervous Tension
Weaning substitute for
hard drugs
Natural Antacid
Gastritis
( Aloe vera with no aluminium)
Indigestion
Parsley
Uro-genital tract infection
( Petroselinum sativum )
Retention of urine
Dropsy
Sinusitis
Sorethroat
Horseradish
Coughs
( Cochlearia armoracia )
Sinus problems
With simple explanation on the use of honey as a
blood alkalizer, antiseptic and a nutrient and advice to avoid the
" 4 white perils " : white sugar,white flour, white rice and " white
powder "- a local term for heroin,
Page 6
I have contrived to reduce a substantial amount of pre-
scribed analgesics,cough mixtures,sedatives,steriods and
antibiotics using the simple adaptogens in my practice.
Holistic Medicine
Holistic medicine is based on the principle that
Nature created the human body in perfect balance and
that sickness is the result of interference with the
equilibrium due to inappropriate nourishment. Nature's
food supply furnishes the elements that would restore
the balanced co-ordination of the various bodily functions.
The herbs and herbal products in relation to health and treat
-ment of diseases must meet the requirements as a Resistance Builder, Repair Agent and a Recovery Product to build
sturdy
minds and bodies in esoteric Yin-Yang proportions. The essence of a plant is in its totality. The healing harmony
of the Whole is not
the same as that of the sum of its parts. An herb is a seed plant
devoid of woody tissue which dies completely after flowering or
is a plant valued for medicinal properties or for its sweet smell
or taste. Lin Yutang stated :
" What is good for the
body is medicine and at the same time, food. "
I am very impressed
with WHO's definition of Holistic Health ( Physical, Mental and Spiritual ).
" Health is a state of COMPLETE
physical, mental and
social well-being and not merely the ABSENCE of disease or
infirmity. "
The Meaning of Disease
Human life and health
depend on very delicately
Page 7
adjusted chemical reactions both inside and outside the
billions of cells in the body. Energy is required for its
its integral organization. This is possible with the correct
chemical combination of the elements from the outer
environment through the we eat, the air we breathe
and the fluids we drink. Health is maintained by an optimum
supply of oxygen with nutrients and removal of wastes.
This is made possible by the " River of Life ", the blood
stream and tissue fluids which form Claude Bernard's
" milieu interieur ". The human body through homeostatic
mechanisms, is self-cleansing, self-protecting and self-
healing. Why then man continues to suffer with more side
effects using modern medication and amenities ? Is auto-
intoxication, a concept founded by Dr. Senator in 1888, a
self-poisoning process due to toxic build-up of metabolites
generated by gastrointestinal bacteria, the result of our
ignorance of nutritional science or due to sheer indifference
to natural elements that ensure our health and survival ?
The secret to man's health and survival is well illustrated
by Dr. Alex Carell of Rockefellow Insitute
for medical
research in USA, who made medical history with his classical
experiment with embryonic chicken heart tissue which survived
for 29 years when the nutrient solution was daily changed but
died one day when it was neglected.
Living cells survive
indefinitely when the supply of nutrients and the removal of
wastes is balanced. Ill-health or breakdown of the functional
capacity of the body is due to defective osmosis at the cellular
level by waste precipitation of "
cell cinders " ( German ) or
" cell carbon " ( English ) which are altered metabolic wastes
such as uric acid, carbonic acid, cholesterol, chlorine and calcium
carbonate blocking the diffusion process across the porous
membrane. This waste infusion is the outcome of abnormal
bowel activity with release of their toxic waste by putrifaction
in the gut by the mutating gut bacterial flora. Health is regained
by detoxification, a cleansing process whereby the obstructive
matter " cell carbon " is removed, thus re-establishing osmotic
efficiency and balanced chemistry. A chemico-physiological
restoration of cellular health also requires an infinitesimal
supply of " cell-salts "
Page 8
which are absorbed minerals, according to the father of
cell salt therapy, Wilheim Schussler MD. These cell salts
acting synergistically with other body chemicals, activate
structures that make the person and form the personality,
are the " living forces " that repair hurts
and revitalise
the body.
Louis Pasteur, the French chemist,discovered germs
during his experimentation on formentation. His discovery
was initially rejected but was later enthusiastically excepted
when the one-germ one-disease model was fashioned to order
with its immense potential for commercial exploitation. In
1914, Dr Rosenow, associate of the Mayo Foundation, the most
eminent bacteriologist then, shattered the foundation of the
serum and drug industries with the results of painstaking
experimentation. The Rosenow experiments, verifying the
conclusions of Bechamp and others, showed that there exists no
specific bacteria. The extant bacteria are the genotypic and
phenotypic variants with marked
capacity to change their
properties to ensure survival in an unpredictable environment.
Bacterial variation occurs
selectively, modifying the microscopic,
colonial, nutritional, biochemical, antigenic, pathogenic
and drug
sensitive attributes of the bacterium, when there is an alteration
in the condition, nutrition and temperature of the environment.
The phenomenon of bacterial variation is observed in our every-
day practice.
1. The development of
resistance to escalating/under dosage
regimen
by mutant strains. ( acquired resistance )
2. The development of multiple
resistance to drugs
( Infective
transfer of Resistance or R factor
from
resistant to sensitive strains )
3. The proliferation of pathogenic
microbes after a single
or combined antimicrobial course, when the vitamin
synthesizing
commensals in the gut, the normal flora in
the
respiratory tract and in the skin are eliminated
(
Superinfection )
4. Temporary acquired resistance
to drugs by bacteria
in
dormant or non-metabolizing state.
Persister
Page 9
state in anti-tubercular chemotherapy.
5. The substitution of drug sensitive bacteria
and re-
infection of surface
wounds or burns by resistant
strains with R Factor
in hospitalised patients.
( Nosocomial cross-infection )
6. Reversion to incomplete drug sensitivity
by previous
-ly resistant strains
when the drug was removed for
some time. ( Mutational
reversion )
Man's
constitution ,the immune system in particular,
determines the pathogenicity of the microbes. His susceptibility
to microbial infection due to an impaired immune system, is
increased with a degenerated body damaged by free radicles
generated by environmental pollutants. The HIV-related Acquired
Immune Deficiency Syndrome ( AIDS ) is an example. The negative
sero-conversion of a non-reactor after a course of vaccination
and the late sero-conversion of a so-called " chronic carrier ",
indicate a dysfunctioning immune system and indirectly record
the consequences of nutritional defects due to pollutant interference.
Quoting A. Milne [ New Zealand Medical Journal 14 Dec '88 ]
" The immunising potency of hepatitis
B Vaccine is not related
directly to the quantity of antigen. It depends, instead, on the tertiary
structuring of the antigen that specified its quality. "
To this I would like to add that
given the immunologically potent
antigen, optimum seroconversion also depends on an unimpaired
immune system.
The Re-awakening
Rejecting
the holistic concept, orthodox medicine is complacent
to be in its technological cocoon but not oblivious to the health hazards
that modern development has brought in its wake. The Western re-awaken
-ing did not find the East dozing. While orthodox medicine slumbers, a
great deal of East-West holistic research data has accumulated.
Page 10
Mother Nature, the guardian of these secrets of ageless wisdom
keeps them locked in dormancy. The first stirrings in the re-awaken
-ing have brought exciting results in the form of potency guaranteed
herbs. The latter has great potential in clinical management of diseases.
While their orthodox contemporaries were using sophisticated
instruments and machines for specialised experiments, the eclectic
physicians were busy doing basic cell counts and test-tube research.
The holistic research data bequeathed to us recorded in parchments,
scrolls and documents, often hidden in caves and secret places, may
be the solution for controlling the pathological processess generated
by the environmental pollutants. Herbalism through the ages has
hallowed the use of these potency guaranteed herbs, which are
scientifically validated. More healing secrets are locked in Nature's
repertoire of herbal wisdom.
Bilbery (Vaccinium myrtillus)
Active constituents: Anthocyanosides - Cyandine, Halvidine,
Delphynidine, Petunidine and Peonidine.
Therapeutic research :
1. Ophthamology
2. Obstetrics
Therapeutic action:
1. Vision disorders
a. Nyctalopia
b. Hemeralopia
c. Eye-strain
d. Vascular retinal disturbances
e. Cataracts
f. Diabetes-induced glaucoma
g. Myopia
2. Vascular disorders
a. Varicose veins
b. Thrombosis
c. Renal haematuria
d. Hypertension
e. Purpuras
Page 11
f.
Arteriosclerosis
Milk
Thistle ( Silybum marianum )
Active
constituents : Silymarin comprising of 3 flavonoids
( Silybin, Silydianin and Silychristin )
Therapeutic
research :
1.
Amanita mushroom poisoning
2. Liver disease
Therfapeutic
action :
1. Liver disease
a. Poisoning
b. Cirrhosis
c. Hepatitis
d. Fatty degeneration
2. Detoxification
a. Air-borne toxins
b. Water-borne toxins
c. Food-borne toxins
3. Alcohol abuse
4. Drug abuse
Gingko ( Gingko biloba )
Active
constituents: Flavoglycosides and Quecetin
Therapeutic
research :
1. Vascular effects
2. Proctology
3. Mental and behavioral effects
4. Alzheimer's disease
Therapeutic
action :
1. Vascular insufficiency
a. Cerebral
b. Crural
c. Arterial
d. Veinous
e. Venular
f. Arteriolar
2. Platelet Aggregation Inhibition
Page 12
4. Inner ear problems
a. Vertigo
b. Tinnitus
c. Hearing loss
5. Proctology
6. Effects on neurophysiology
7. Mental and behavioral manifestations
a. Dementia
b. Alzheimer's Disease Syndrome
Echinacea ( Echinacea augustifolia )
Active constituents: Echinacosides
Therapeutic research:
1. Antibiotic action
a.
Streptococci
b. Staphylococcus aureus
c. Trichomonas vaginalis
d. Candida albicans
2. Connective tissue stabilization
a. Echinacin B ( Polysaccharide )
b. Inhibition of hyaluronidase
c.
Stabilization of H-system
3. Connective Tissue Repair
4. Stimulation of macrophage and T-
cell activity
5. Cancer
a. Walker's carcinoma
b. Lymphatic leukaemia
6. Properdin
7. Interferon
induction
Butcher's Broom ( Ruscus aculeatus )
Active constituents: Ruscogenins
Therapeutic research:
1. Proctology
2. Circulatory disorders
3. Post-operative recovery
Page 13
Therapeutic action:
1. Protology
a. Haeorroids
b. Proctitis
c. Pruritus ani
d. Anal fissures
2. Phebology
a. Varicose Veins
b. Varices
c. Chiblains
d. Postthrombotic syndrome
e. Varicophlebitis
f. Varicose ulcers
3. Ophthalmology
a. Diabetic retinopathy
b. Retinal haemorrhage
4. Gynaecology
a. Menstrual problems
b. Cramps of pregnancy
c. Varicose veins of pregnancy
( Milk Legs )
Tumeric ( Curcuma longa )
Active constituents: Curumin
Therapeutic research:
1. Liver protection
2. Antibiotic activity
3. Anti-inflammatory effects
4. Arthritis
5. Cholagogue
6. Gall Bladder Disease
Therapeutic action:
1. Digestion
2. Cholagogue
3. Weight loss
4. Snake bite
Centella ( Centella asiatica: Madagascara variety )
Active constituents: Asiaticosides and other triterpenes
Therapeutic research:
Page 14
1. Sclerosis
2. Skin ulcers
3. Gynaecology
4. Ear,Nose & Throat
5. Cellulitis
6. Venous insufficciency and Phebitis
Therapeutic action:
1. Skin injuries
a. Open skin sores/cellulitis
b. Wounds
c.Tears
d. Surgical incisions
e. Ulcers
2. Confinement
a. Bed sores
b. Phlebitis
3. Venous insufficiency
a. Varices
b. Leg cramps
c.
Oedema
Ginseng ( Panax Ginseng )
Active constituents: Ginsenosides
1.
Rb1 group:
a. Rb1
b. Rb2
c. Rbc
d. Rbd
2. Reg1 group:
a. Rg1
b. Re
c. Rf
d. Rg2
Therapeutic research:
1.
Stress
2. Hypothalamo pituitary adrenal axis
3. Cardiovascular effects
4. Digestive effects
5. Immunity
Page 15
6. Geriactrics
Therapeutic action:
1. Stress
2. Venous tension
3.
Depression
4. Hypotension
5. Hypertension
6. Anaemia
7. Asthma
8. Indigestion
9. Fatigue/Exhaustion
10. Arthritis
These potency guaranteed herbs and herbal products
are usually taken in the capsular form and are non-toxic. How-
ever, heavy dosage of Echinacea augustifolia may index induce
temporary infertility in the male; hyaluronidase is one of the
three enzymes attached to the acromosal membrane located on
the head of the spermatozoon.
Nature's laboratory
The chemical laboratory cannot replace or equal
Nature's alchemical laboratory. Abiogenesis, the doctrine of
origination of life from inert material is advocated by the
synthetic world health,rejuvenation and increased life-span are
possible with synthetic food and supplements. I shated Ann
Wigmore's belief in Biogenesis ( Hippocrates' Health Institute ,
USA ) that living thing are only produced from living things.
The biochemict can imitate an egg but he cannot make it hatch.
In fact, the egg, so is the milk and honey, is herbal at one stage
in Nature's Biological Laboratory. Natural vitamins, under
polarised light, show optical rotation; synthethic vitamins are
optically inactive. What the human body cannot synthesize,
( Vitamin C, Linoleic acid ) Nature has catered
for in the natural
form in Man's diet. We lost the gene for
the hepatic synthesis
of Ascorbate from glucose some 60 millions ago .
The genetic defect:
Enzymatic absence of l-gulonolactone
oxidase during the final stage of
Page 16
-ion of 1-gulonolacton into ascorbate, forms the basis of
Dr. irwin Stone's hypothesis : Hypoascorbemia, a very low
blood level of ascorfbic acid. Dr. Stone, a pioneer in vitamin
research and application, contended that
Vitamin C is a
pseudovityamin and that the superior bioavailability or vitamin
C resides in its hepatic metabolite. Esterified
vitamin C, a
synthetic, attains a faster blood level and
maintains a higher
blood levvel than traditional vitamin C, contains similar hepatic
metabolites. Only future research will reveal whether the effective
bioavailability of Ester vitamin C is due to its complementing or
enhancing property on natural hepatic metabolites.
Linus Pauling's
megadosing recommendation for the common cold is considerably
reduced using esterified C. Natural comcomitants of vitamin C
commonly encountered are the bioflavanoids, collectively called
vitamin P, are:
Quecetin Anthocyanidin Hesperidin
Catechin Khellin Asculetine
Rutin Astragelin Luteolin
The
bioflanoids are particularly effective at oxidative
protection of vitamin C, thus,greatly potentiating and maximizing
its action. Besides chlorophyll and carotenoids, the flavanoids are
the most common pigments in the plant kingdom. Apart from their
widespread biologically active anti-oxidant
property, the bio-
flavonoids also have the following attributes:
1. Anti-tumour
3. Anti-viral
2. Anti-bacterial
4. Anti-hyaluronidase
5. Immunostimulating 6. Anti-hepatotoxic
7. Capillary permiability stabilizing
8. Haemostatic
and many more of other scientifically proven activities. Nature
has taught me that natural ingradients are preferable to
synthetic ones.
The body's anti-oxidant system
Page 17
The body's anti-oxidant system of free radical
scavengers
comprises of nutrients which re-establish the equil-
brium
between cellular destruction and regeneration in the form
of:
1. Enzymes:
a. Super Oxide Dismutase
b. Glutathione peroxidase
2.Co-enzymes:
a. Copper
b.Zinc
c. Manganese
d. Selenium
3. Sulphur-containing amino-acids
a. Methionine
b. Cysteine
4. Vitamins
a. Vitamin A ( Beta - carotene )
b. Viatamin E
c. Vitamin C
d. Vitamin B3
e. Vitamin B6
Super Oxide Dismutase ( SOD ) is synthesized in the
body
from its precursors:
1. Zinc
2. Manganese
3. B6
It is ineffective orally as assimilation is poor. Super
Oxide
Dismutase has been used successively intravenously to neutral
-ise
the excessive superoxides in the cells generated by the environ-
mental
and dietary pollutants. Hence the body has to be adequately
replenished
to offset the destructive action of free radicals produced
by
the ubiquitous pollutants. Perhaps , it is only Nature that has the
capability
to contain then devastating effects of our environment.
Factually,
our artificial
Page 18
lifestyle and modern industrialization are responsible
for a new sick syndrome which modern science cannot coup
with : Oxygen starvation. Nobel Price winner, Otto Warburg
MD, showed more than fifty years ago that cancer is a
process of cell mutation on the cellular level caused by
oxygen deprivation and is not virus-induced. Cancer thrives
in a hypoxic environment : His
theory still stands uncontra-
dicted to-date.
The erythrocyte levels of the antioxidant enzymes SOD and GPx, and serum levels of antioxidants vitamins β
-carotene and β -tocopherol were estimated in various types of brain tumors, and were compared with the levels
in controls. Statistically significant (P<.001) diminished levels of β - carotene, β -tocopherol, SOD
and GPx, were observed in all the brain tumor patients as compared to controls. Malignant tumor also showed a relative decrease
in antioxidant levels as compared to benign tumors. Comparison of histopathological sections of brain tumors also suggested
a inverse relationship between antioxidant level and grades of malignancy. Marked decrease in antioxidant levels may have
a role in genesis of considerable oxidative stress in brain tumors. Further more, the degree of decline in antioxidant levels
may indicate severity of malignancy in brain tumors.
Medical challenge : Environmental pollutants
What challenges medicine to-day is not cancer,
arthritis,cardiovascular disease, allergy or diabetes. The
real challenge medicine and allied sciences have to face
is the " free radical fall-out
" from such " nuclear-waste"
as food preservatives, pesticides, insecticides, toxic chemicals,
medications, ultra-violet radiation, alcohol, cigarrete smoke
and in fact from any combustion source, the sun's rays, any
burnt item including the " burning of glucose " with oxygen.
These free radicals enter
the body through the fluids we
imbibe, the food we partake,the air we in hale and radiation.
Research studies have shown that these oxidizing free radicals
are causatively linked with all aging degenerative diseases. Free
radicals are incomplete molecules with unpaired electrical charge,
which set up a chain reaction by conversion and reaction on coming
in contact with body tissues. Cells damaged by free radicals
persist as intracellular lipofuscin pigments which impede oxygen
flow into cells. Lipofuscin pigments increase with age. The immune
system is put at great
risk when free radicals damage the genetic
code in the cells, with consequences of mutation and cancer. Many
of the diaseases classified as " idiopathic ", " idiotoxic ",
" iatrogenic ", " chronic " or " terminal " are the inexorable
pathological processess caused
by the " free radical fall-out ".
Holistic medicine calls for a more aggressive evaluation with due
emphasis on environmental pollutants or such medical entities
rather than just a mere classification. The harsh re-awakening
from holistic dormancy and the peep-look Nature's merciful bounty
should make us realise the immediate deficiencies in our
pharmaceutical defence. The ho-
Page 19
listic research material that has been collected so pain
-stakingly by our visionary eclectic peers through the
ages, should deserve a better reception by the medical
establishment. It is hoped that the guardians of health
realise what price mankind has paid and has to pay in the
name of technological progress. The world is not the same again
shrouded and clouded by environmental pollutants. We
are living in a precarious world. My essay is a mere whisper
lost in the roar of the medical establishment. But it is
still an effort worth trying : Helping to get research
started in adaptogenic biopharmaceutics in Malaysia. Man's
intellectual forces have forged very sophisticated instruments
and machines, no less in the medical field.
Bowing with an appeal
What I think is a feasible approach to the
practice of holistic medicine, under the circumstances, in my
area of practice is in no way an attempt to depreciate orthodox
medicine. When the alert for the typhoid spread was given sometime
in April 1990 and with no vaccine at hand. I turned to Nature
for help. Honey,besides being a first class nutrient and a
mild systemic alkalizer, has also antibiotic properties.
It is bactericidal to Salmonella bacilli. Kahang with the adjacent
forests and estates, has a ready supply of natural honey for
its inhabitants. Cost-effective commercial brands are also available
in the sundry shops (though less effective ). I prescribe honey as a
mild systemic alkalizer, as a prophylactic and as a nutrient for my patients in Kahang. I also
abserve the protocol issued by the MMA.
Holistic medicine found me in the process of re-
discovering my medical roots and recovering from the heady
technological revolution which came near to destroying traditional
medicine. Malaysia is a multi-racial country with many colourful
traditions. Unfortunately, scientifically validated herbal
medicine has never been taught in medical institutions. In our
hurry to achieve technological excellence to be at par with
other developed countries, we should not forget our humble
medical
Page 20
origins. In the splendour of computerised marvels at
diagnostics and treatment, we should not be so souless
as to crush the humble plant under our feet. Scientific
validation of herbal extracts has shown that potency
guaranteed constituents can effect results which surgery
or computerised sophistry may not be able to reach.
When Dr. TCN Singh from Annamalai University, South
India, demonstrated that music by resonance could induce
a greater agricultural yield,which is stored up energy
food produced by the accelerated vibration of the plant
molecules induced by musical sound waves, particularly
those from high-pitched violin or from soprano voices,
genetic transference of this high-yielding trait has also been
observed. Botanical research has revealed that planmts are
capable of reacting to human behaviour with " feelings ".
This Krishna-inspired departmental head in
Botany paved the way for international research ( Europe and America ) where at least
scientists now dared to ask whether corn has ears for music.
To extrapolate from this musical experience, through resonance,
Nature's omnipotent energy transformer, why can't specific healing
requirements be structured in musical composition for vibratory
transmission to plants for medicinal production? It is not impossible
in these days of computerised genetic engineering.
"
The greatest service to any country is to add a useful
plant to its culture ."
-Thomas Jefferson
When man is despair of his outer world, he begins slowly
to
look within his microcosm to search for relief. This is the re-
awakening of holistic medicine, which treates the "inner" cause
of disease to relieve the " outer symptoms ". The Human Void is
One which defines the esoteric Yin-Yang philosophy where life
is balanced energy in its myraid forms.
Man's dependence on plant life is in more ways than one for
sustenane and health. The botanical side
Page 21
of man has need of stored up energy produced by the
resonance
of two different wave-lengths of light ( red and blue ), during
photo-synthesis. Hence, the energy in plant food is the photo-
synthetic equivalent of a music chord. Whether in man or in a
plant, physiologically or abstractly, life is a melody.
An introductory course on herbal medicine for
doctors may be a good start for those who are reawakening.
This is a mere suggestion. This essay may prove to be a big
disappointment to my teachers, a headache to my peers and a
piece of fantasy to my colleagues. For me, school may be hard but
it is a lot easier than growing up. And we comphrehend little. How
could a part hear the Whole or a Note, the Melody ?
" In your explorations of the realms of Science, for
undiscovered truths, and unknown and untried agents, seek not
for potent poisons, but stop and examine the simple plant under
your feet, for in it wonderful curative properties may be found. "
- L.Stanton, PD & D.E. Smith ,MD Presented at the
Annual Meeting of the Eclectic Medical Society, June 12 1887
References:
1. Louise Tenny
Today's Herbal Health
Woodlands 1983
2. J.V. Cerney A.B., D.M. , D.P.M
Handbook of Unusual and unorthodox
Healing Methods ( Reward Edition 1977 )
Parker Publishing Company, Inc,
West Hyack, New York
3. M.Q. Garten, D.O.
The secrets of a Naturopathic Doctor
( Reward Edition 1976 )
Parker Publishing Company, Inc.
Acknowledgement;
I extend my heart-felt thanks to all those supportive Companies
that had supplied me herbal nutriceuticals for research
in remote regions when I most needed them.I thank
fellow Homeopaths, the world over, in particular Professor Dr. Nik Omar from Kota
Baru, Kelantan, Malaysia for their kind and humane gesture, in deeds (supplies) and writings (books) when I most
needed them when I was in attendance of Mother Nature's tutorials on the Homeopathic Principle, at the fringes
of the Malaysian Rainforests, which the Master, Dr. Hahnemann, in the 6th edition of " Organon of Medicine "
described as VITAL ENERGY.
I thank PathLab ( Malaysia ) for the supply and delivery of nutriceuticals. I reciprocated
this kind gesture when I
worked for a year as the medical officer in Century Medical
center,for examination of foreign workers, Kuala lumpur, Malaysia,after my sojourn
in Southern Malaysia. And
many thanks to 21st Century, Drug House of Austrialia,for the many herbal samples.
I fed guppies and local fishes
with the chlorella and spirulina samples supplied. You
are pioneers. To-day, these phytonutrients are incorporated in petfish food. Mother
nature nutures
all her creations.
Dr.FHLew
Kuala Selangor, Malaysia
Handphone : 0176963793
|